



Dear administration of medical schools in the United States,
As a senior in high school in the process of mapping out my future, I am confronting questions that feel both exciting and daunting. I know that after undergraduate school I would like to pursue medicine and continue my studies through attending medical school.
Yet, with knowing that is the path I want to take comes a growing awareness of the financial realities tied to it. The likelihood of accumulating significant debt has caused me to think twice, not because I don’t want to have a commitment to medicine, but because the cost of becoming a physician is already shaping my decisions as I apply to colleges as a pre-med genetics major.
As I am going through this process, I am beginning to see how the cost of medical education influences access long before students ever step into a medical school classroom.
In an April 2025 article for Ms. Magazine, Tiffany Lemuz reveals how medical school debt affects students long before they ever become physicians, particularly women with caregiving responsibilities. As a single mother in medical school, Lemuz describes preparing for board exams in carpool lines, squeezing in study sessions during lunch breaks, and reviewing notes late at night while her son slept beside her.
These moments reflect not a lack of dedication but an effort to meet the demands of a system that offers little flexibility. Despite fulfilling every expectation placed on future doctors, Lemuz was told she might not be able to graduate, not because of academic failure or burnout but because she had reached a federal lifetime loan cap that does not account for parenthood, low income, or inflation.
The possibility that years of sacrifice could end not in a medical degree but in forced withdrawal underscores how unforgiving the system can be. Lemuz’s experience exposes how medical education has been designed around students without caregiving responsibilities or financial instability, leaving others to carry both professional ambition and personal responsibility alone. Through this lived experience, medical school debt emerges not simply as a financial obstacle, but as a deeply human issue shaped by access, gender, and equity.
In a 2021 article for the Petrie-Flom Center at Harvard Law School, Leah Pierson explains that the average medical student now graduates with more than $215,000 in debt from medical school alone, a figure that reflects decades of unchecked tuition increases. Over the past seventy years, the cost of a medical degree has risen by approximately 750 percent, with student debt more than quadrupling since the late 1970s.
This trend is made immediately visible in a graph published by the Education Data Initiative, which shows average medical school debt steadily increasing over time, reaching $216,659 among new indebted graduates in 2025. The visual reinforces that rising debt is not the result of isolated personal choices, but a consistent, national pattern.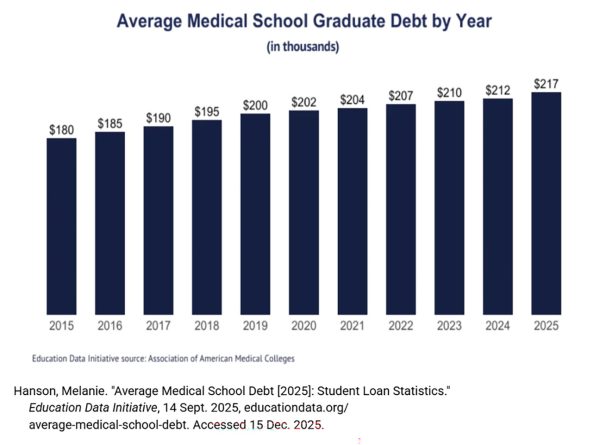
Together, these sources show that medical school debt extends far beyond finances. Higher debt is linked to physician burnout and mental health challenges and pushes graduates toward higher-paying specialties instead of primary care or underserved communities.
Although most physicians borrow to attend medical school, nearly one-third still owe more than $250,000, highlighting the lasting nature of this burden. Without changes to tuition structures or degree pathways, the cost of medical education will continue to determine who is able to become a physician and who is pushed out before they ever begin.
Some argue that medical school debt can be managed through individual decision-making. In a 2024 article for the American Medical Association, Brendan Murphy explains that students who attend public, in-state medical schools often graduate with significantly less debt, saving an estimated $73,400 compared to peers at private institutions. Murphy cites data showing that the median four-year cost of attendance for in-state public medical schools is substantially lower than that of private schools, suggesting that strategic school selection can reduce financial strain.
While this argument is reasonable, it assumes that all students have equal access to high-quality in-state programs. Many aspiring physicians seek specialized training, research opportunities, or clinical placements that may not be available at their state institutions, and some states lack well-resourced public medical schools altogether. As a result, students are often forced to choose between affordability and opportunity.
Medical school debt is shaping who is able to pursue medicine long before students ever enter a classroom, and its consequences reach far beyond individual borrowers. When the cost of medical education discourages capable, compassionate students from becoming physicians or pushes future doctors away from underserved communities, the entire healthcare system is affected. As administrators of medical schools, you all have the power to change this trajectory.
By reevaluating tuition structures, degree timelines, and financial support systems, you and your institutions can help ensure that access to medicine is determined by ability and commitment, not by financial circumstance. The future of healthcare depends on who is allowed to enter the profession, and that responsibility cannot rest on students alone.
Sincerely,
Ava Carbonara